The pathologic and radiologic spectrum of ILD associated with Ig deficiency is remarkably wide. This is reminiscent of collagen vascular diseases, in which the same disease and the same immune abnormalities can be associated with many different types of ILD. With the exception of granulomatous pneumonitis, which could not be confidently catogo-rized in subject 15, all diffuse ILD and the chronic postinflammatory pneumonitis previously related to CVID are now shown to coexist with IgG isotype deficiency. In addition, NSIP, apparently not reported before in CVID, may also be associated with IgGSC deficiency Canadian Pharmacy. 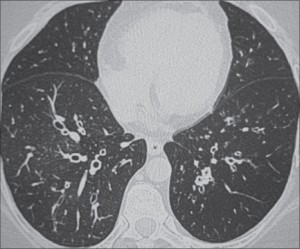
Two of the ILD cases mentioned in this article deserve special mention. Neutrophil alveolitis represents a nonspecific inflammatory reaction. It may be associated with a clear chest radiograph (eg, systemic lupus erythematosus), radiologic ILD, or CVID with bronchiectasis in free interval. Pleading for interstitial involvement, despite a normal HT scan finding of the chest, was an occasionally positive Ga scan finding (subjects 2, 3, and 4) and mild restrictive abnormality on pulmonary function testing.
Bronchiectasis with chronic postinfectious pneumonitis was described in antibody deficiency by means of high-resolution HT scan and labeled interstitial disease, chronic lung disease, fibrosis , the lesions are complex, involving the bronchi, alveoli, and the interstitium. In agreement with the literature, bronchiectasis with chronic interstitial pneumonitis was usually diagnosed by HT scan (subjects 16 through 21) and only exceptionally by biopsy (subject 11). Radiologic and pathologic aspects (subject 11) suggest that BOOP may constitute an important part of chronic pneumonitis.
In several patients (subjects 22 through 29), ILD seems to be related to a specific etiopathogenic entity, but the observed low Ig levels may still participate in the genesis of interstitial inflammation. In the patient with systemic lupus erythematosus, a low IgG1 is totally unexpected since IgG1, the isotype carrying most of the antinuclear activity, is usually increased rather than decreased. In the patient with myotonic dystrophy, a low IgG1 resulting from its increased catabolism in this disease was expected, but the bibasilar interstitial infiltrates
were not.